
Surfing Voluntarily in Dreams – The Science of Lucid Dreaming
Have you ever experienced of achieving conscious awareness of dreaming while the dream is still happening? This phenomenon is known as lucid dreaming (LD). LD has become increasingly well-known in recent years with the representations in popular media such as the sci-fi movie “Inception”. While LD often occurs spontaneously, there are reports on deliberately induction of LD1. The underlying reason for volitionally inducing LD is partly due to the belief that LD would promote psychological well-being2. The current article aims to review the practical evaluation of LD and to highlight the physiological nature and health impacts of LD.
Prevalence of LD
The meta-analysis by Saunders et al (2016), which included 34 studies in the period of 1966 to 2016, reported that 55% of adults have experienced at least one LD, and 23% of them experienced LD at least once per month3. Likewise, a previous study in Germany by Voss et al (2012) involving 694 students aged between 6 and 19 suggested that 51.9% of the participating students reported to have had at least one lucid episode. The results further indicated that LD was more frequent among young children, whereas the frequency of LD decreased gradually reaching a low frequency after the age of 16 (Figure 1)4. This observation thus hints the association between the natural occurrence of LD and brain maturation.

Figure 1. Relative prevalence of frequent LD4
Inducing LD
LD can be tempting in the sense that one can enter a state of consciousness in which he/she can perform feats not possible in real life, such as flying, by exerting control over dream scenarios. Thus, there are research interests on inducing LD volitionally. Stumbrys et al (2012) summarised that there are 3 main categories of technique for inducing LD, namely cognitive techniques, external stimulation techniques, and miscellaneous techniques5. Combining the wake-up-back- to-bed (WBTB) sleep protocol and mnemonic induction of lucid dreams (MILD) is one of the cognitive techniques for inducing LD. Practically, the participant is awakened after 6 hours of sleep from a subsequent rapid eye movement (REM) period and keep awake for 30 or 60 min, during which he/she needs to practice MILD, which involves recalling their dreams and identifying all possible dream signs. Then the participant returns to bed for a morning sleep period6. External stimulation techniques involve stimuli such as flashing lights presented during REM sleep, whereas miscellaneous techniques include LD-inducing drugs and supplements5. Although former systematic review by Stumbrys et al (2012) suggested that none of the induction techniques were verified to induce lucid dreams reliably and consistently5, Aspy (2020) reported that the predictors of successful LD induction included superior general dream recall and the ability to fall asleep within 10 minutes of completing the LD induction procedures7.
Visualising LD
Besides induction techniques, the physiology of LD has attracted interests of researchers and psychologists. The pioneer works of practical evaluation on physiological parameters associated with LD were established in the late 1970s. Ogilvie et al (1982) evaluated the association between lucidity and alpha activity measured by electroencephalogram (EEG) during REM sleep. The findings reflected that alpha feedback had no effect on lucidity8. Nonetheless, a more recent work by Holzinger et al (2006) reported an increased power in the low beta frequency range (13-19 Hz) in parietal regions for lucid compared to non-lucid REM sleep. The ratio of frontal to parietal beta-1 activity was 1 to 1.16 in non-lucid and 1 to 1.77 in lucid dreaming. Notably, the left parietal lobe is considered to be related to semantic understanding and self-awareness9. Moreover, Voss et al (2009) showed that increased activity in the gamma band in the frontal and frontolateral region during lucid as compared to baseline REM sleep (Figure 2)10.
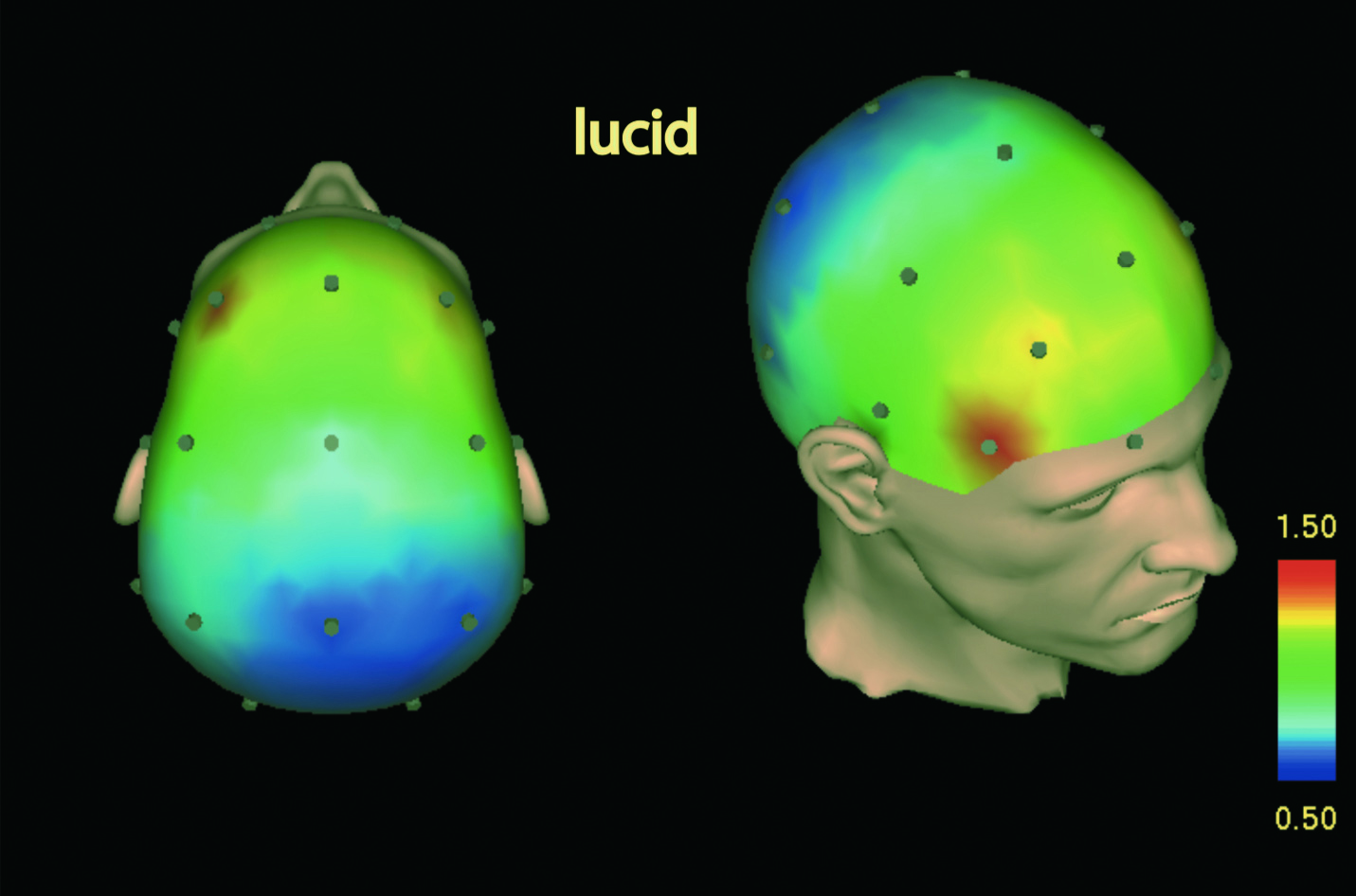

Figure 2. Gamma 40-Hz standardised current source densities (CSD) power during lucid and baseline REM10
In recent investigations on LD, comprehensive measurements of brain waves, heart rate, breathing, as well as eye and body movements during sleeping are conducted by polysomnography (PSG) to register sleep stages. PSG recording normally includes EEG, electroocculogram (EOG), submental electromyogram (EMG), and electrocardiogram (ECG). Particularly, LD has been demonstrated to be objectively verifiable through volitional eye movement signals which can be recorded in the EOG6.
Of note, a combined EEG/fMRI case study by Dresler et al (2012) revealed that increased blood-oxygen-level dependent (BOLD) signals were observed in anterior prefrontal cortex (aPFC), bilateral inferior parietal lobule (IPL), precuneus and inferior/middle temporal gyrus (ITG/MTG) during LD compared to non-lucid REM sleep (Figure 3)11.
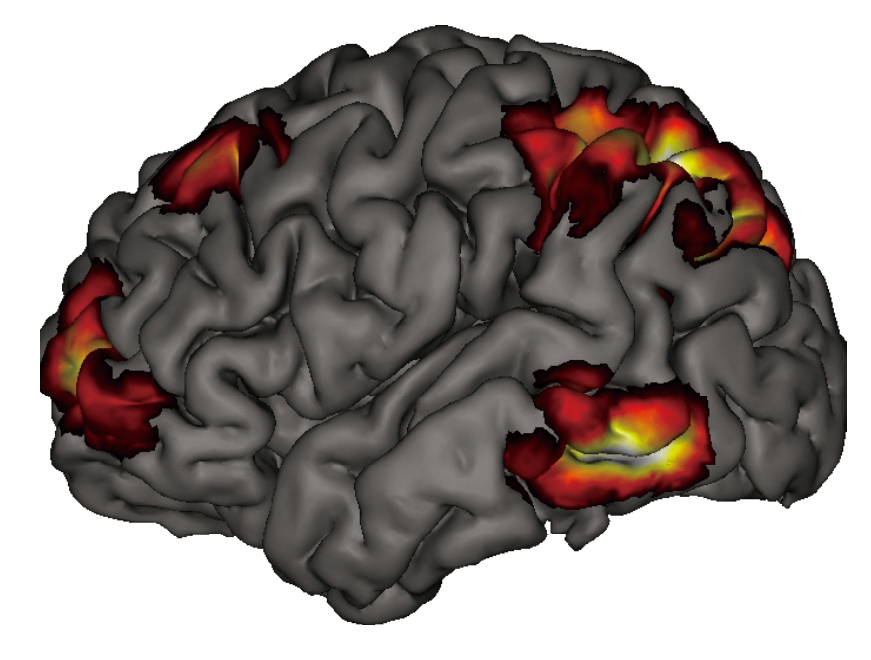
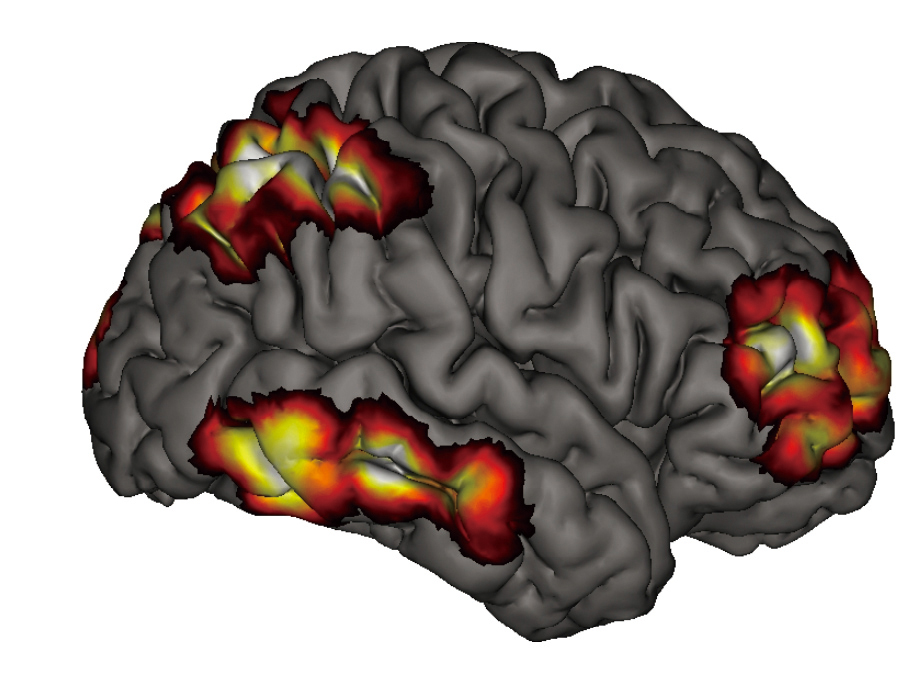
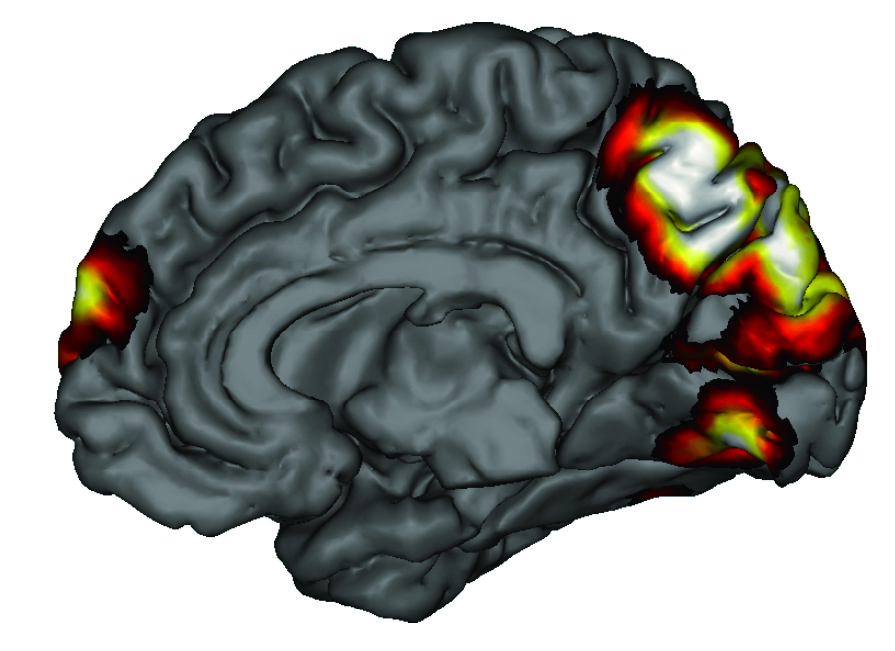
Figure 3. Increased BOLD activity related to LD11
Neurological Explanation of LD
PSG and neuroimaging techniques allow to visualise the characteristic patterns of regional brain activity during sleep. For instance, during non-lucid REM sleep, neural activity in the brain stem, thalamus, amygdala, and extrastriate temporo-occipital cortices increases, whereas the dorsolateral prefrontal cortex and the precuneus show deactivation. This pattern of neural activity has been suggested to reflect visual hallucinations, emotional intensifications, and cognitive abnormalities typically experienced in dreams12.
In LD, higher cognitive capabilities are regained leading to the awareness of the dreaming state. The wake-like intellectual clarity would likely be associated with the neural activations in frontal and frontolateral regions as reflected by quantitative EEG10. While the dorsolateral prefrontal cortex is suggested to underlie a wide range of higher cognitive capacities, activation in the region in combination with parietal lobules was observed during LD11. As bilateral frontopolar areas are related to the evaluation of one’s own thoughts and feelings, increased activation of these regions in LD would contribute to the regaining of awareness during sleep. Essentially, the strongest increase in activation during lucid compared to non-lucid REM sleep was observed in the precuneus, which has been implicated in self-referential processing, such as first-person perspective13. This might, at least partially, explain the reflection on one’s own state of mind in LD. Summarising the findings in EEG and neuroimaging, the reactivation of brain regions which are deactivated during normal sleep would be associated with the recovery of reflective cognitive capabilities leading to the onset of LD.
The Health Impacts of Lucid Dreams
While LD is characterised by the regain of awareness during dreaming state, it is questionable whether LD would disrupt sleep quality and adversely impact health. A recent cross-sectional study by Schadow et al (2018), which included a student sample (n = 444) and a population-based sample (n = 1380), showed that the frequency of LD was significantly associated with poor sleep quality. However, the association disappeared when adjusted by the frequency of nightmare14. Thus, LD might not directly impair sleep quality but alternative factors would contribute to the adverse outcome. Interestingly, while recurrent nightmares cause significant distress and impairment in occupational and social functioning, Macêdo et al (2019) suggested that LD may be a feasible aid in the treatment of patients with nightmares through minimising their frequency, intensity and psychological distress by allowing the patients to re-signify the dream scenes15.
On the other hand, an analysis of dream diary in the course of a LD induction study by Schredl et al (2019) involving 149 participants indicated no negative effect of having LD on the feeling of being refreshed in the morning compared to nights with the recall of a non-lucid dream2. On the contrary, the results indicated the feeling of being refreshed is positively related to the occurrence of LD2.
Although there are opinions suggesting LD would enhance well-being and can potentially be applied as treatment, opposing findings on LD for disrupting sleep exist. Aviram and Soffer-Dudek (2018) evaluated the characteristics of LD and their relations with symptomatology. The results demonstrated that LD frequency was unrelated to psychopathology, but LD intensity, and positive LD emotions were inversely associated with several psychopathological symptoms. Moreover, the results suggested that the use of deliberate induction techniques was positively associated with psychopathology and sleep problems16.
In summary, LD appears to enhance well-being in some senses. Nonetheless, the potential risk associated with LD, particularly the deliberate induction, has to be taken into account. Yet, further investigations would provide more comprehensive insights on the physiological and psychological impacts of LD. Last but not least, wish you have a sweet dream tonight, regardless of lucidity.
References
1. LaBerge et al. Dreaming 1995; 5: 159–68. 2. Schredl et al. Clocks & Sleep 2020; 2: 54. 3. Saunders et al. Conscious Cogn 2016; 43: 197–215. 4. Voss et al. J Sleep Res 2012; 21: 634–42. 5. Stumbrys et al. Conscious Cogn 2012; 21: 1456–75. 6. Erlacher et al. Front Psychol 2020; 11: 1383. 7. Aspy. Front Psychol 2020; 11. DOI:10.3389/FPSYG.2020.01746. 8. Ogilvie et al. Percept Mot Skills 1982; 55: 795–808. 9. Holzinger et al. Dreaming 2006; 16: 88–95. 10. Voss et al. Sleep 2009; 32: 1191. 11. Dresler et al. Sleep 2012; 35: 1017. 12. Hobson et al. Nat Rev Neurosci 2002 39 2002; 3: 679–93. 13. Cavanna et al. Brain 2006; 129: 564–83. 14. Schadow et al. Int J Dream Res 2018; 11: 154–9. 15. deMacêdo et al. Front Psychol 2019; 10: 2618. 16. Aviram et al. Front Psychol 2018; 9. DOI:10.3389/FPSYG.2018.00384/FULL.









