Drink It Or Leave It?
A Review on the Association between Coffee Consumption and Bone Health
Coffee is one of the most commonly consumed beverage worldwide. Having a coffee break is relaxing, whereas coffee consumption has been reported to have potential health benefits, such as prevention of type 2 diabetes mellitus, cardiovascular disease, certain types of cancer, and Parkinson’s disease1. On the contrary, there are research works reporting the harmful effects of coffee, such as increased blood pressure, serum total and low-density lipoprotein cholesterol concentrations, and plasma homocysteine concentrations2. In particular, the association between coffee consumption and bone quality has been heavily investigated. Nonetheless, conclusive findings are yet to be established. The objective of this article is to review the effects of coffee consumption on bone health.
Osteoporosis - The Disturbed Balance between Bone Formation and Resorption
Osteoporosis is the condition in which a low bone mass and altered micro-architecture of the bone leads to increased risk of fracture. Besides osteoporosis caused by other health problems, osteoporotic condition is usually associated with aging and decreased gonadal function, such as decreased levels of estrogen3. Moreover, lifestyle factors, including cigarette smoking, inadequate calcium and vitamin D intake, excessive alcohol consumption, physical inactivity, use of medications such as glucocorticoids, and etc4., are reported to be risk factors for osteoporosis.
Skeletal growth and repair occur through bone-remodeling which is a tightly regulated process. The normal bone mass is maintained during remodeling, based on the balance between bone formation and bone resorption. The bone-remodeling cycle begins with the resorption phase, which is mediated by the action of osteoclasts (bone-eating cells), followed by the formation phase, during which mature osteoblasts (bone-building cells) deposit an organic matrix for subsequent mineralisation3. In case the rate of bone resorption outweigh that of bone formation, depletion of bone mass and disruption of skeletal microarchitecture would occur leading to skeletal fragility.
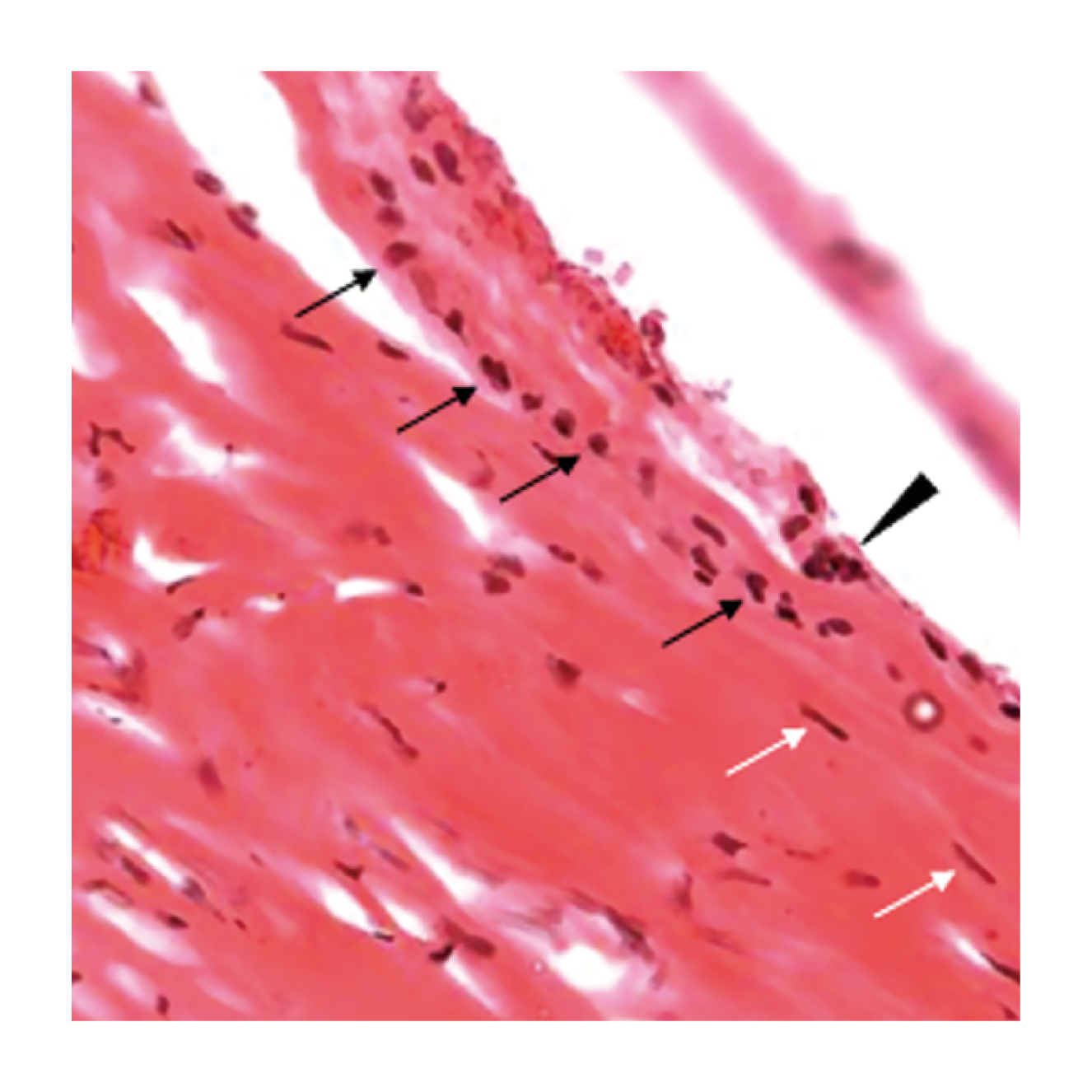
Figure 1. Osteoclasts, osteoblasts and bone lining cells, bone lining cells (white arrow) and Osteoblasts (black arrow) laying down bone matrix along bone surface. Osteoclast (arrowhead) is characterised by its multinucleated structure and abundant cytoplasm.
Coffee Eats Up Your Bone
Caffeine (1,3,7-trimethylxanthine) is a pharmacologically active component of many foods, beverages, dietary supplements, and drugs. While caffeinated beverages, like coffee, have been consumed for centuries, there are increasing varieties of caffeine-containing products, such as energy drinks. The concern on caffeine safety has been emerged with the increasing global consumption of caffeine-containing products.
In view of the impact on bone, a community-based study by Connor (1994), which involved 980 postmenopausal women aged 50 to 98 years, demonstrated a statistically significant graded association between increasing lifetime intake of caffeinated coffee and decreasing bone mineral density (BMD) at both the hip and spine5. On the other hand, a cross-sectional study involved 489 women aged 65-77 years by Rapuri et al (2001) reported that women with high caffeine intakes (>300 mg/day) had significantly higher rates of bone loss (% change: -1.90) at the spine than those with low caffeine intakes (% change: +1.19, p = 0.038)6. More recently, another cross-sectional study (2016) conducted in 270 women between 40 and 48 years indicated that caffeine intake (>300 mg/day) was associated with low BMD (odds ratio: 2.6, p = 0.03)7. Thus, coffee consumption, at least at higher intakes, would be associated with lower BMD, particularly among postmenopausal women.
Coffee Is Not Harmful but May Protect against Bone Loss
While some reports suggested coffee consumption to be detrimental to bone quality, there are other findings indicating that coffee is not associated with bone loss, or even beneficial to bone health. For instance, the longitudinal population-based study by Hallström et al (2013), which involved 61,433 women born in 1914-1948 followed up from 1987 through 2008 reported that there was no evidence of a higher rate of any fracture (hazard ratio per 200 ml coffee = 0.99) or hip fracture (hazard ratio per 200 mL coffee = 0.97) with increasing coffee consumption. The results further indicated that a high coffee intake (≥4 cups daily) versus a low intake (<1 cup daily) was associated with a 2%-4% lower bone density, depending on site (P < 0.001), but the odds ratio for osteoporosis was only 1.28 (Figure 2)8. Hence, the findings suggested that high coffee consumption was associated with a small reduction in bone density that did not translate into an increased risk of fracture.
Interestingly, the meta-analysis by Lee et al (2014), which included 253,514 participants with 12,939 fracture cases from 9 cohort and 6 case-control studies, demonstrated different effects of coffee consumption respectively in men and women. The results suggested that daily consumption of coffee is associated with an increased risk of fractures in women (estimated relative risk [RR] of fractures at the highest level of coffee consumption = 1.14) and a contrasting decreased risk in men (RR = 0.76). In the dose-response analysis, the pooled RRs of fractures in women who consumed 2 and 8 cups of coffee per day were 1.02 and 1.54, respectively (Figure 3)2.
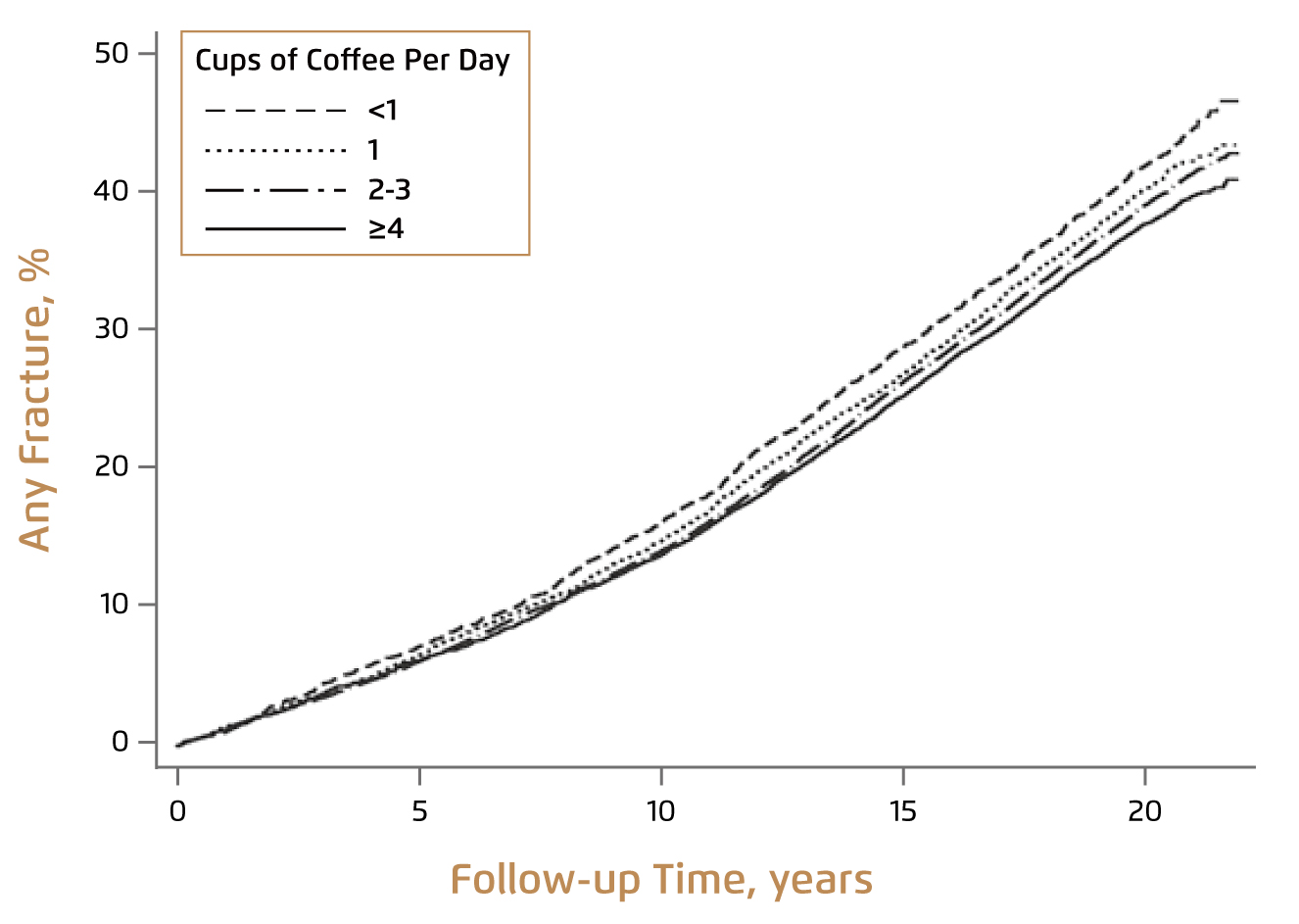
Figure 2. Age-adjusted incidences of any fracture for various categories of coffee consumption8
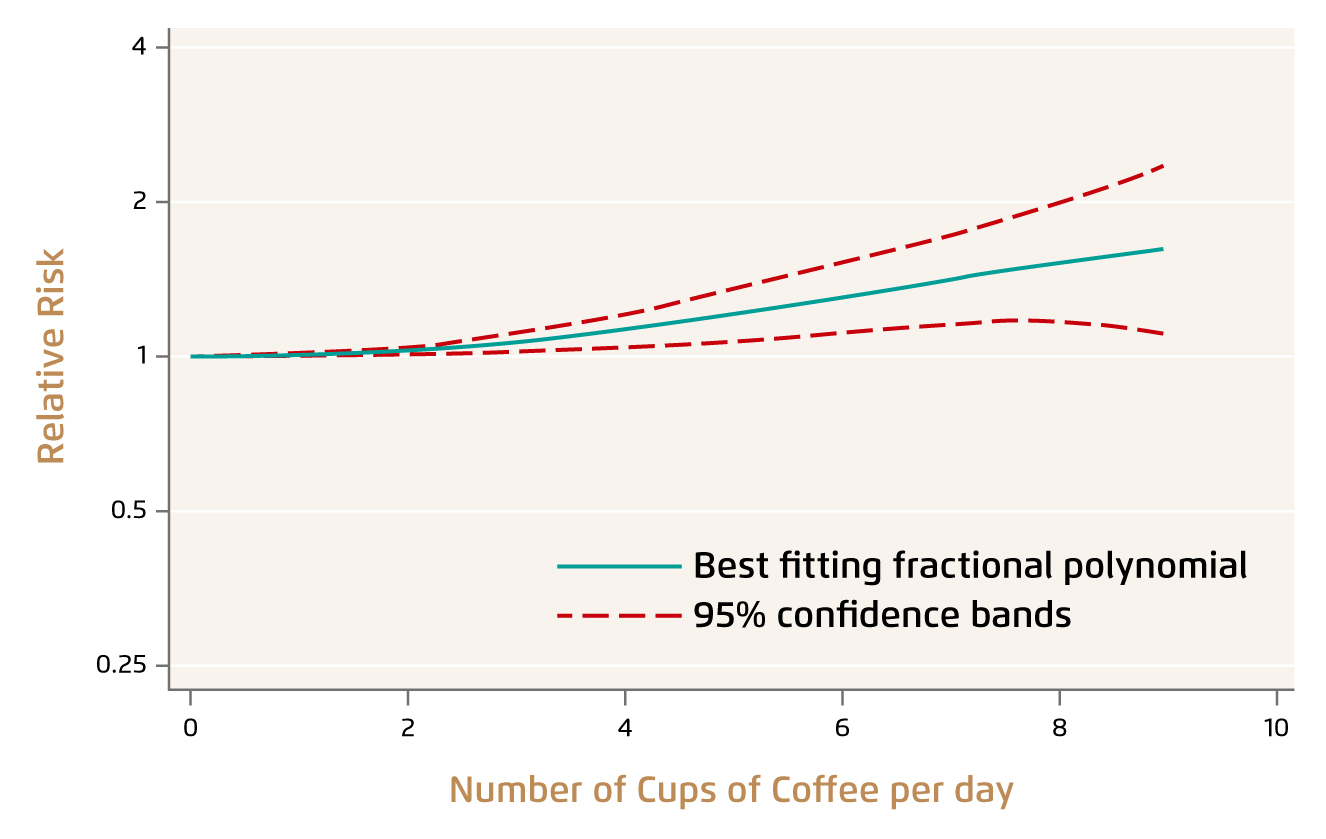
Figure 3. Dose-response relationship between coffee consumption and the risk of fractures in women2
On the other hand, a recent longitudinal study in Taiwan by Chang et al (2018), involving 1,195 men and 1,487 women (706 premenopausal and 781 postmenopausal), demonstrated that medium (drank coffee 1-2 times per week, 240 ml each time) and high (3 time or more) coffee drinking were associated with higher T-scores. However, significant results were observed only among high drinkers (p = 0.0038). In the stratified analysis, significant positive associations between T-score and coffee drinking were observed among male high drinkers (p = 0.0067), premenopausal medium female drinkers (p = 0.0355) and premenopausal high female drinkers (p = 0.0152)9. The results thus suggested that coffee drinking was significantly associated with higher T-scores hence, a lower risk of osteoporosis in men and premenopausal women.
Too Much of a Good Thing Can Be Bad
In reality, assessing the impacts of coffee consumption on bone quality is very challenging. As described above, the coffee intake could be varied in different trials. Also, factors including gender, age, menopause status, and etc. would affect the outcomes as well. Notably, the caffeine contents can be different even for the same amount of coffee beverage, which further creates variation among studies. Moreover, the technical procedures for evaluating outcomes varied among studies. These factors partially explain the inconsistent results among former studies. Nonetheless, there are emerging evidence supporting that moderate coffee consumption would offer various physiological benefits, including reduced risk of fracture1. Higher intake of coffee, however, has been suggested to be associated with osteoporosis, particularly in postmenopausal women. Hence, to reduce risk of osteoporosis, adequate physical exercise and calcium intake, as well as moderate coffee consumption is advisable.
References
1. Poole et al. BMJ 2017; 359: j5024. 2. Lee et al. Bone 2014; 63: 20-8. 3. Lau and Guo. J Osteoporos 2011. DOI:10.4061/2011/293808. 4. Pisani et al. World J Orthop 2016; 7: 171. 5. Barrett et al. JAMA 1994; 271: 280-3. 6. Rapuri et al. Am J Clin Nutr 2001; 74: 694-700. 7. Huitrón-Bravo et al. BMC Musculoskelet Disord 2016; 17. DOI:10.1186/S12891-016-1273-7. 8. Hallström et al. Am J Epidemiol 2013; 178: 898-909. 9. Chang et al. BMC Public Health 2018; 18. DOI:10.1186/S12889-018-6168-0.