Council Member
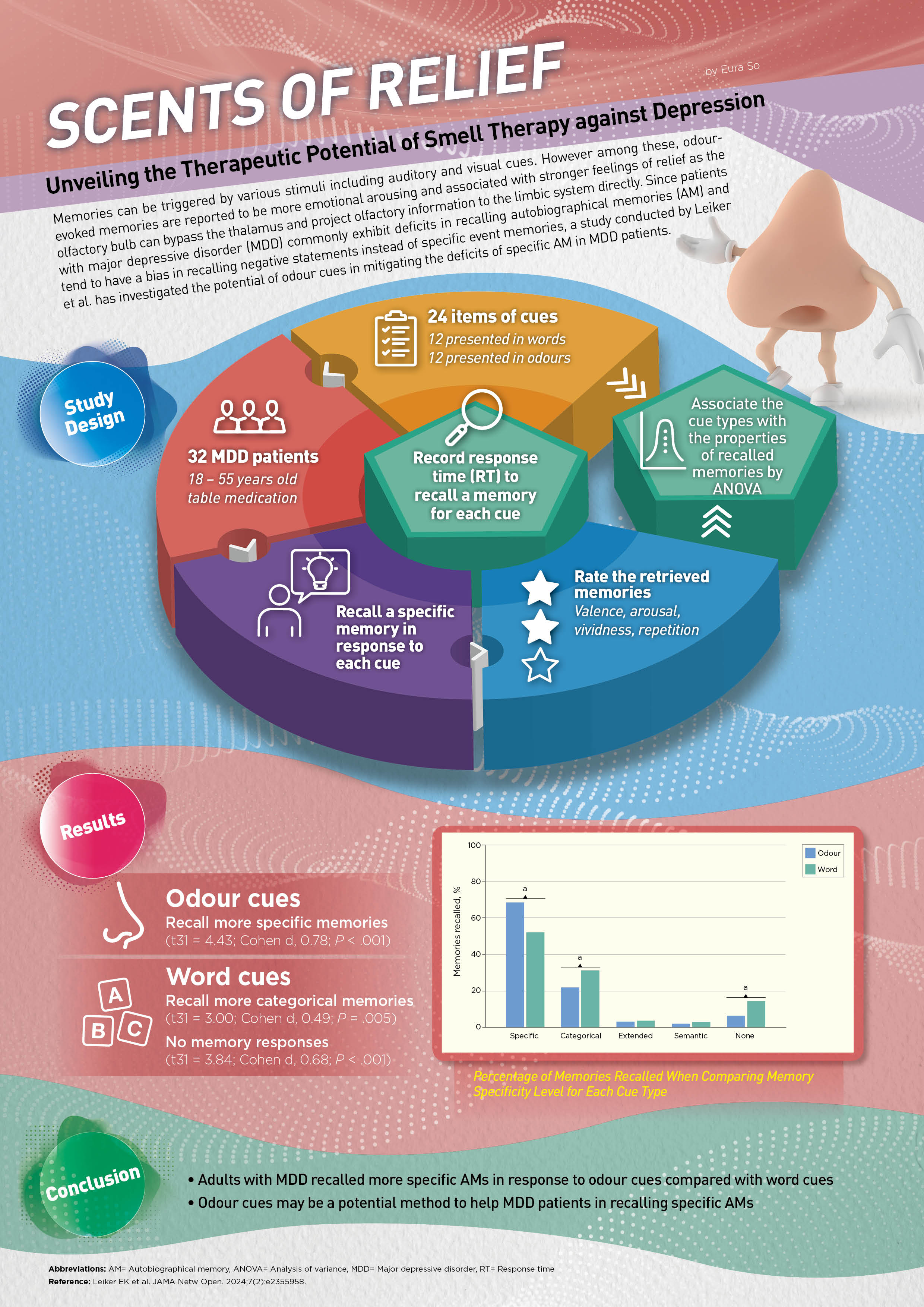
Hong Kong Kidney Foundation
and Hong Kong Society of Nephrology
The epidemic of non-communicable diseases, including obesity, type 2 diabetes mellitus (DM), cardiovascular disease (CVD), and chronic kidney disease (CKD), is escalating and widely acknowledged in industrialized nations, while the interconnection of these diseases has been collectively conceptualized as the Cardiovascular-Kidney-Metabolic (CKM) syndrome1. The conceptualization of CKM syndrome enables a multidisciplinary approach in the risk stratification, early prevention, and treatment of the vicious circle generated by the interaction among disease components. In addition to specialist care, the involvement of primary care is vital for providing holistic care for patients with CKM syndrome. Accordingly, in a recent symposium titled “Cardiovascular-Kidney-Metabolic (CKM) syndrome: Why and How It Matters for Every Primary Care Physician” jointly organized by the Hong Kong Society of Nephrology (HKSN), the Hong Kong Kidney Foundation (HKKF), and the Hong Kong Association of Renal Nurses (HKARN), Dr. Chow Kai Ming was invited to discuss the pathophysiology of CKM syndrome and practical issues in managing the disease.
Dr. Chow emphasized that metabolic disorders often occur together. For instance, approximately 25%–40% of patients with heart failure (HF) have DM, and approximately 40%–50% of patients with HF have CKD. Both DM and CKD are associated with increased risk of incident HF. Importantly, the combination of these 3 comorbidities is associated with a substantially increased risk for hospitalization and mortality2. Given that patients would suffer from complications in various organs, Dr. Chow highlighted that multidisciplinary care is essential in managing CKM syndrome. In particular, primary care physicians are the initial point of care for patients with various chronic diseases. “There may be limited treatment options available if the patients were referred to specialty care after advanced complications have developed,” Dr. Chow expressed. Thus, the roles of primary care physicians in identifying CKM patients and facilitating early treatment are crucial.
Given the complex interaction among the disease conditions, managing CKM syndrome is clinically challenging. However, Dr. Chow further noted that the challenge can be intensified by clinical inertia of physicians, which refers to the phenomenon of failing to initiate or intensify treatment for patients who are not achieving evidence-based therapeutic goals3. Accordingly, regular review and optimization of the management protocol for CKM patients is required.
The clustering of condition under the umbrella of CKM syndrome not only highlights the risk of comorbid conditions but also establishes a holistic framework that incorporates screening, staging, and management to facilitate the early identification of potential CKM-related events4. In view of the conglomeration of metabolic disorders, Dr. Chow noted that CKM syndrome cannot be managed by a single specialty alone, whereas primary care physicians who have the patients’ comprehensive clinical information are helpful in providing holistic care. Notably, a recent consensus recommendation on the management of CKD in Hong Kong advocated that primary care plays a core role in the strategies to improve patient awareness of CKD, adherence to treatment, and achievement of CKD care goals5.
In evaluating the risk of CVD, Dr. Chow specifically recommended the PREVENTTM risk calculator formulated by the American Heart Association (AHA) in 2023, which includes urine albumin-creatinine ratio (ACR), body mass index (BMI), and glomerular filtration rate (GFR) as predictors6. Remarkably, Dr. Chow emphasized that the ACR test is cost-effective for accurately estimating the risk of CKM syndrome.
Dr. Chow illustrated the clinical significance of ACR test with the case of a female patient aged 60 years, who was a non-smoker and had hypertension with a history of gout. The patient was non-diabetic, with fasting glucose of 6.2 mmol/L and HbA1c of 5.7%. The cholesterol and LDL-C levels were 4.9 mmol/L and 2.4 mmol/L, respectively. Also, normal computed tomography coronary angiography (CTCA) is reported. Based on the AHA 2013 formula, which focuses on CV parameters only, the estimated 10-year CVD risk for the patient was 6.5%, suggesting statin therapy was not needed. In contrast, using the PREVENTTM risk calculator with the ACR test result, the estimated CVD risk was significantly higher (>10%), indicating the need for statin treatment. In this regard, the updated calculation of risk coupled with the appropriate clinical test will guide the appropriate treatment decision.
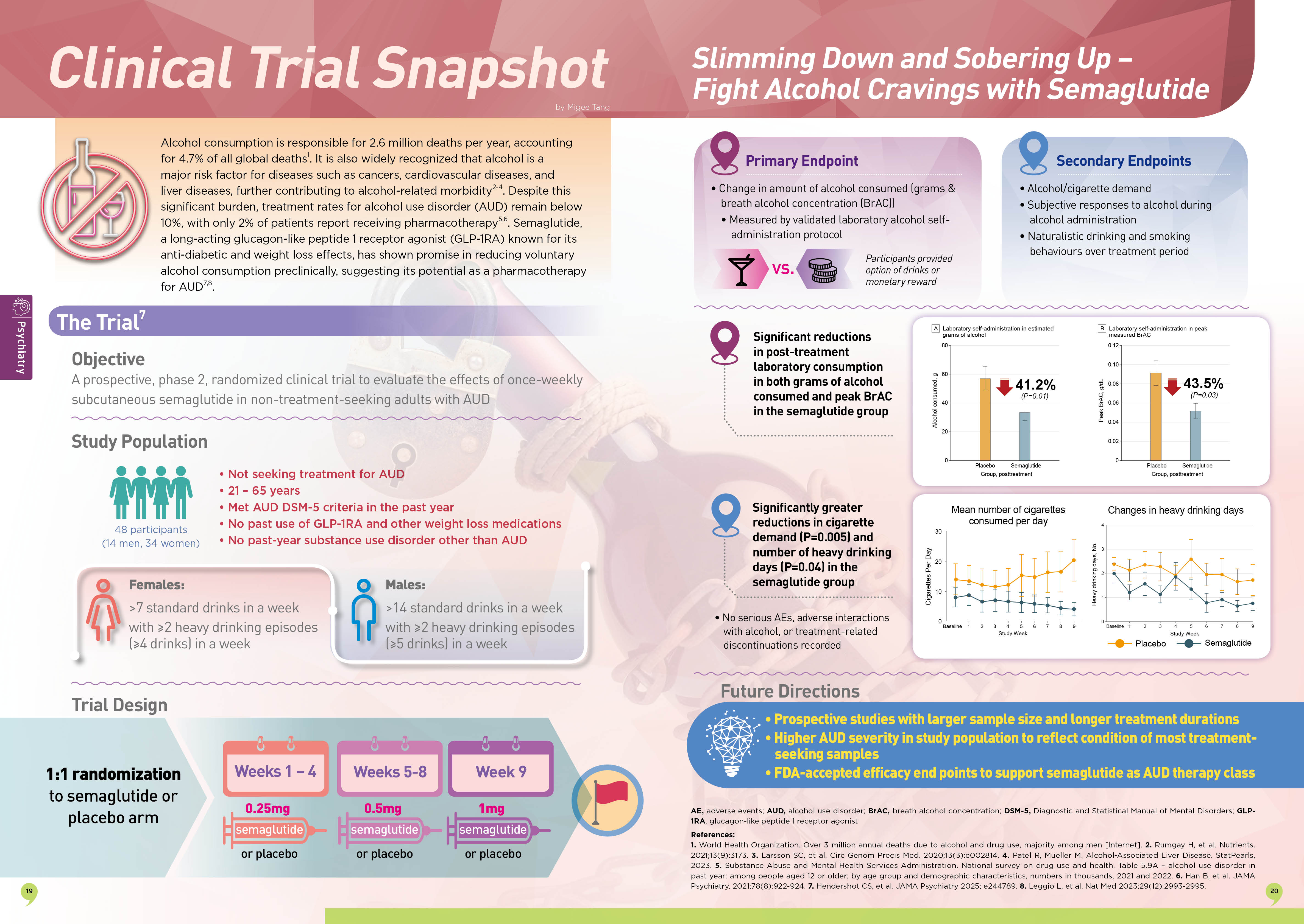
Moreover, an analysis of the data from NHANES III by Afkarian et al. (2013) revealed that the presence of albuminuria significantly increased mortality risk among DM patients (Figure 1)7. Hence, albuminuria has been included as one of the markers of kidney damage in the KDIGO 2024 Clinical Practice Guideline8.
 Syndrome Why and How It Matters for Every Primary Care Physician/F1 R1_VPulse_HKKF CKM lecture_text _cathy20251103_1004 (1)-3.jpg)
Figure 1: 10-year mortality in DM by kidney disease manifestation7
Despite effective clinical tests and treatments being available, it takes an average of 17 years to move them from clinical evidence to daily practice9. For instance, while an ACR test is crucial for guiding evidence-based treatments to mitigate CKD progression and CV morbidity, a meta-analysis by Shin et al. (2021) suggested that the ACR screening rate was only 35.1% in diabetes and 4.1% in hypertension10. Dr. Chow highlighted that about 60% of local DM patients in 4 general medical clinics under the Hospital Authority (HA) had not been screened for urine ACR in 2022. This reflects that improving the detection of CKM syndrome by enhancing the ACR screening rate is urgently needed. “I place 10-20 urine bottles in a “kidney dish” on my consultation desk everyday as a visual cue reminding myself to test ACR for my patients,” Dr. Chow suggested.
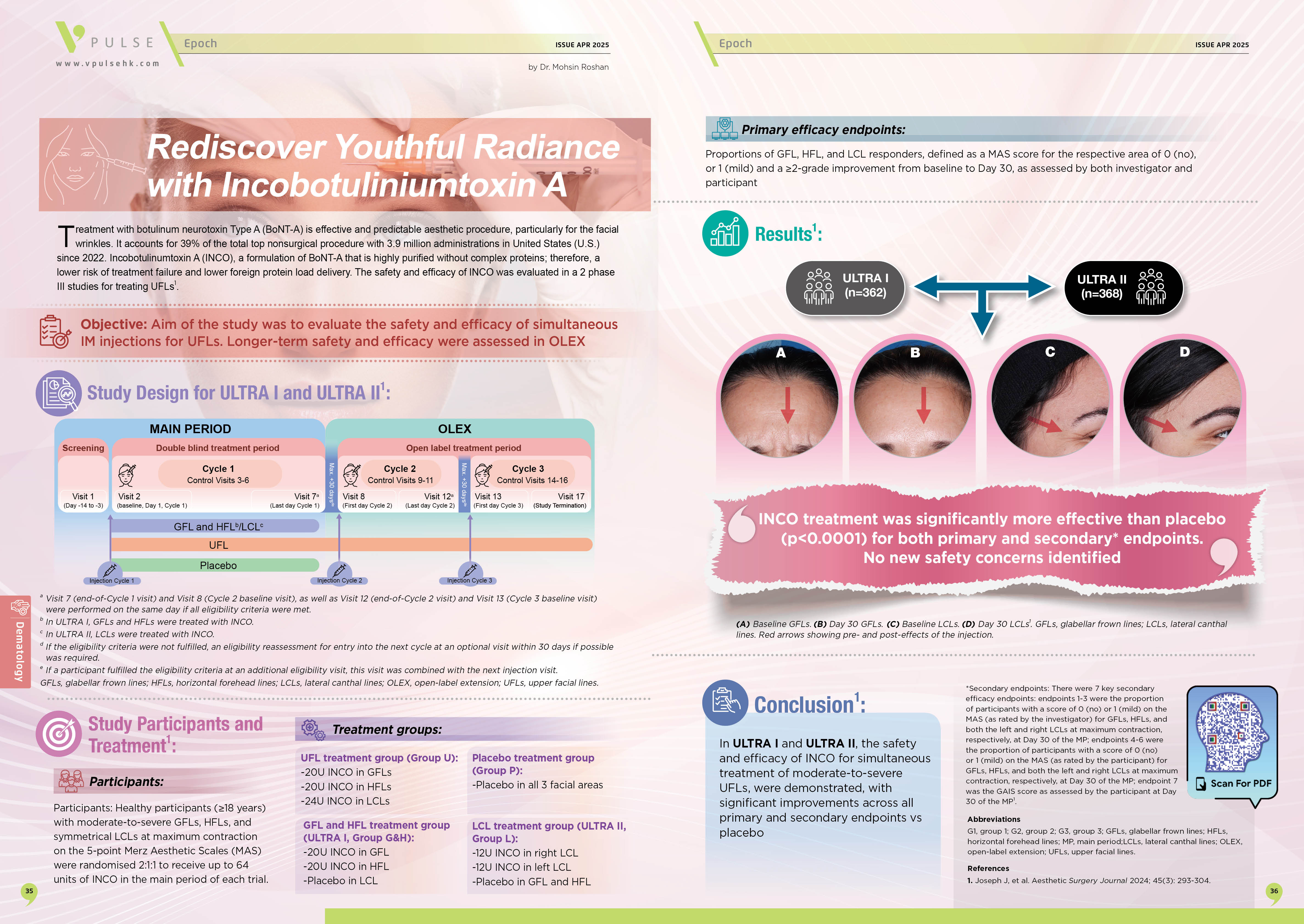
Apart from ACR screening, therapeutic inertia can be another clinical problem. Dr. Chow particularly addressed the issue of intensive control in managing hypertension. According to the SPRINT trial, which involved 9,361 with a systolic blood pressure of 130 mmHg or higher and an increased cardiovascular risk, intensive control targeting a systolic blood pressure (SBP) of <120 mmHg resulted in significantly lower rates of fatal and nonfatal major CV events (Figure 2) and death from any cause as compared to standard control, which targeted systolic blood pressure at 140 mmHg11. Moreover, a subgroup analysis of the SPRINT trial indicated that intensive control of SBP to <120 mmHg resulted in significantly lower rates of fatal and nonfatal major cardiovascular events and death from any cause. Remarkably, the impact of intensive control was more pronounced among older patients with higher frailty12. Hence, Dr. Chow commented that a lenient hypertension treatment for frail patients is not advisable.
 Syndrome Why and How It Matters for Every Primary Care Physician/F2 R1_VPulse_HKKF CKM lecture_text _cathy20251103_1004 (1)-4.jpg)
Figure 2: Primary outcome at 1 year in the SPRINT trial11
More recently, a meta-analysis of 6 randomized controlled trials (RCTs) accounting for 80,220 participants by Guo et al. (2025) confirmed that, after a median follow-up of 3.2 years, intensive blood pressure control provides a net benefit between the reduction in CV events and the increase in adverse events, including renal events, compared with standard control13. “Although there may be potential harm for intensive control, it has to be 3 times more adverse events to outweigh the harm from its benefits. Thus, withholding intensive blood pressure control is not good for patients,” Dr. Chow commented.
To demonstrate the clinical management of patients with established CKM syndrome, Dr. Chow shared the case of another female patient aged 77 years who had been diabetic since 1997 and had triple-vessel coronary disease requiring coronary artery bypass graft (CABG) in 2010. The patient’s left ventricular ejection fraction (LVEF) was 45% and eGFR was 33 ml/min/1.73m2. The patient was initially treated with losartan, carvedilol, linagliptin, and rosuvastatin since 2015. Upon the addition of empagliflozin to the treatment regimen, the urine ACR decreased from 28.7 mg/mmol in July 2019 to 9.96 mg/mmol in July 2023. Finerenone was then prescribed and the urine ACR was further reduced to 4.40 mg/mmol in April 2024. “Even for advanced CKM diseases, there are still many effective treatment options available,” Dr. Chow noted.
Together with renin-angiotensin system (RAS) blockade, sodium-glucose co-transporter-2 inhibitors (SGLT2i), non-steroidal mineralocorticoid receptor antagonists (ns-MRA), and glucagon-like receptor-1 receptor agonists (GLP-1RAs) are collectively the 4 pillars of pharmacotherapies in CKM management. Importantly, the KDIGO Clinical Practice Guidelines recommend initiating an angiotensin-converting enzyme inhibitor (ACEi) or an angiotensin II receptor blocker (ARB) for patients with DM, hypertension, and albuminuria, and the medications should be titrated to the highest approved dose that is tolerated14.
In the patient with established CKM symptoms above, hyperkalemia (serum potassium 5.4 mmol/L) and a serum creatinine of 330 µmol/L were observed after prolonged treatment. In this regard, recent clinical studies suggested that discontinuation of RAS inhibitors in patients with advanced CKD was not associated with favorable outcomes15. On the contrary, the treatment should be continued to control further CKD progression, with monitoring and maneuvers to control potassium level.
In addition to RAS inhibitors, SGLT2i was prescribed to the patient as well. A key recommendation in the updated KDIGO Guidelines is to prescribe SGLT2is for patients with DM, CKD, and eGFR ≥20 mL/min/1.73m2 by virtue of the significantly reduced risk of mortality and extended time to dialysis14. Notably, Dr. Chow stated that an initial reversible decrease in eGFR can be observed after initiating SGLT2i, which is generally not an indication for discontinuing therapy. Requesting renal function test soon after initiating SGLT2i is therefore not a must. “Apart from the patients, the healthcare sector will be benefiting from the saved treatment costs and time associated with SGLT2i treatment,” Dr. Chow opined.
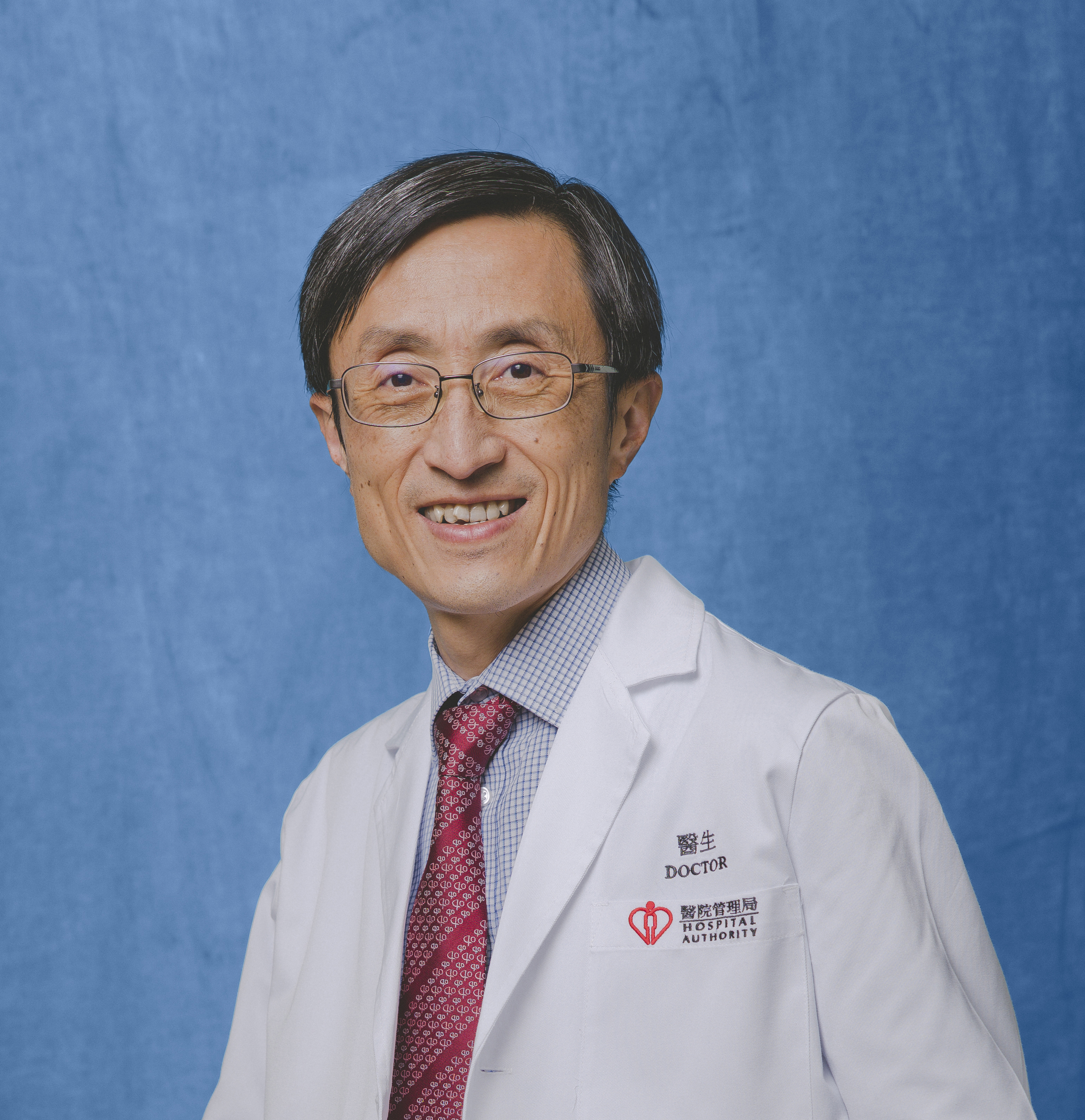
Besides, ns-MRA is a relatively new therapy for managing CKM syndrome. The KDIGO 2024 Guidelines recommend ns-MRA for DM patients with eGFR >25 ml/min/1.73m2, normal serum potassium concentration, and albuminuria (>3 mg/mmol)8. The efficacy of finerenone, a ns-MRA, in reducing CV and kidney events was demonstrated in the FIDELITY pooled analysis (Figure 3A and 3B). Remarkably, finerenone was reported to reduce urine ACR by 30% from baseline to 4 months16. Dr. Chow reminded us to monitor serum potassium at 1 month, then every 4 months, after initiating finerenone. Finerenone should be withheld when serum potassium is >5.5 mmol/L. Interestingly, the recent CONFIDENCE trial by Agarwal et al. (2025), which included patients with CKD and DM, reported that initial therapy with finerenone plus empagliflozin led to a greater reduction in the urinary ACR than either treatment alone17.
 Syndrome Why and How It Matters for Every Primary Care Physician/F3 R1_VPulse_HKKF CKM lecture_text _cathy20251103_1004 (1)-5.jpg)
Figure 3: Time to efficacy outcomes, A) composite CV outcomes, B) composite kidney outcomes16
Remarkably, obesity is one of the parameters included in the PREVENTTM risk calculator6. GLP-1RAs stimulate insulin release in response to glucose load through incretin release. By delaying gastric emptying and effects on the satiety center in the brain, GLP-1RAs provoke weight loss18. In the FLOW trial, which involved 3,533 CKD patients with DM, semaglutide, a GLP-1 RA, significantly reduced the risk of clinically important kidney outcomes and death from CV causes19. Thus, GLP-1 RAs can be considered for obese CKD patients. Furthermore, recent pooled analysis suggested that semaglutide reduced the risk of the combined endpoint of CV death or worsening heart failure events in patients with heart failure with mildly reduced or preserved ejection fraction (HFpEF)20. The results supported the use of semaglutide to reduce the risk of clinical heart failure events in patients with HFpEF.
In summary, Dr. Chow outlined the 5 pillars in CKM management. In addition to the 4 pillars of pharmacotherapies above, statins are the important 5th pillar controlling dyslipidemia. In addition to these 5 pillars, Dr. Chow emphasized the importance of lifestyle modifications, including a low-salt diet, exercise, weight control, and smoking cessation, as the foundation for preventing CKM syndrome. As the final remark, Dr. Chow reminded us to be mindful of clinical inertia in managing CKM syndrome since Stage 0 (no risk factors observed) of the disease.
References
1. Sebastian SA, Padda I, Johal G. Cardiovascular-Kidney-Metabolic (CKM) syndrome: A state-of-the-art review. Curr Probl Cardiol 2024; 49. DOI:10.1016/j.cpcardiol.2023.102344. 2. Vijay K, Neuen BL, Lerma E V. Heart Failure in Patients with Diabetes and Chronic Kidney Disease: Challenges and Opportunities. Cardiorenal Med 2022; 12: 1–10. 3. Lewinski AA, Jazowski SA, Goldstein KM, Whitney C, Bosworth HB, Zullig LL. Intensifying Approaches to Address Clinical Inertia Among Cardiovascular Disease Risk Factors: A Narrative Review. Patient Educ Couns 2022; 105: 3381. 4. Lee CH, Tan G, Tang SCW, et al. Incorporating the cardiovascular-kidney-metabolic health framework into the local healthcare system: a position statement from the Hong Kong College of Physicians. Hong Kong Med J = Xianggang yi xue za zhi 2025; 31: 58–64. 5. Tang SCW, Ho KKL, Ko WWK, et al. Management of chronic kidney disease: a Hong Kong consensus recommendation. Hong Kong Med J = Xianggang yi xue za zhi 2024; 30: 478–87. 6. Khan SS, Matsushita K, Sang Y, et al. Development and Validation of the American Heart Association’s PREVENT Equations. Circulation 2024; 149: 430–49. 7. Afkarian M, Sachs MC, Kestenbaum B, et al. Kidney disease and increased mortality risk in type 2 diabetes. J Am Soc Nephrol 2013; 24: 302–8. 8. Stevens PE, Ahmed SB, Carrero JJ, et al. KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int 2024; 105: S117–314. 9. Luyckx VA, Tuttle KR, Abdellatif D, et al. Mind the gap in kidney care: translating what we know into what we do. Kidney Int 2024; 105: 406–17. 10. Shin JI, Chang AR, Grams ME, et al. Albuminuria Testing in Hypertension and Diabetes: An Individual-Participant Data Meta-Analysis in a Global Consortium. Hypertens (Dallas, Tex 1979) 2021; 78: 1042–52. 11. Wright JT, Williamson JD, Whelton PK, et al. A Randomized Trial of Intensive versus Standard Blood-Pressure Control. N Engl J Med 2015; 373: 2103–16. 12. Williamson JD, Supiano MA, Applegate WB, et al. Intensive vs Standard Blood Pressure Control and Cardiovascular Disease Outcomes in Adults Aged ≥75 Years: A Randomized Clinical Trial. JAMA 2016; 315: 2673–82. 13. Guo X, Sun G, Xu Y, et al. Benefit–harm trade-offs of intensive blood pressure control versus standard blood pressure control on cardiovascular and renal outcomes: an individual participant data analysis of randomised controlled trials. Lancet 2025; 406: 1009–19. 14. KDIGO 2022 Clinical Practice Guideline for Diabetes Management in Chronic Kidney Disease. Kidney Int 2022; 102: S1–127. 15. Bhandari S, Mehta S, Khwaja A, et al. Renin–Angiotensin System Inhibition in Advanced Chronic Kidney Disease. N Engl J Med 2022; 387: 2021–32. 16. Agarwal R, Filippatos G, Pitt B, et al. Cardiovascular and kidney outcomes with finerenone in patients with type 2 diabetes and chronic kidney disease: the FIDELITY pooled analysis. Eur Heart J 2022; 43: 474-484A. 17. Agarwal R, Green JB, Heerspink HJL, et al. Finerenone with Empagliflozin in Chronic Kidney Disease and Type 2 Diabetes. N Engl J Med 2025; 393: 533–43. 18. Agarwal R, Fouque D. The foundation and the four pillars of treatment for cardiorenal protection in people with chronic kidney disease and type 2 diabetes. Nephrol Dial Transplant 2023; 38: 253–7. 19. Perkovic V, Tuttle KR, Rossing P, et al. Effects of Semaglutide on Chronic Kidney Disease in Patients with Type 2 Diabetes. N Engl J Med 2024; 391: 109–21. 20. Kosiborod MN, Deanfield J, Pratley R, et al. Semaglutide versus placebo in patients with heart failure and mildly reduced or preserved ejection fraction: a pooled analysis of the SELECT, FLOW, STEP-HFpEF, and STEP-HFpEF DM randomised trials. Lancet (London, England) 2024; 404: 949–61.