Doctor at the National Health Services (NHS), United Kingdom (UK)
Physical restrains can have a negative impact on patients’ physical and mental health, thus, their use in clinical setting should be reduced1. In addition, little is known internationally about the use of restrains and there are no clear regulations against their use. Hence, they are often used in hospitals for various reasons, particularly as a precautionary measures for patients at risk of falls, or those with cognitive impairment1. Despite this, studies have shown the removal of restrains made no changes to the fall rates, injury rates as well as the therapy disruptions. Moreover, older patients are often put on physical restraints in either nursing homes or during hospital stays and some argue that this creates a number of ethical issues since physical restraints may hinder the ability to be self-reliant, especially in older adults1. Furthermore, the negative outcomes of physician restraint use have often been reported, but very limited research effort has been made to examine whether such practice have any adverse effects on patients’ length of stay (LOS) in hospitals. Therefore, this article will discuss the research findings regarding the use of physical restrains in hospitals, the adverse effects they have on patients’, particularly the older adults.
It is no surprise that the implication of aging population is having a detrimental effect on the economic growth since the working-age population is shrinking, and thereby, putting strain on the healthcare system2. To date, the utilisation of physical restraints is still a widespread practice in clinical setting and has been associated with several physical, as well as psychosocial forms of harm3. For instance, the prevalence of pressure ulcers, joint injuries, or increased risk for delirium are relative complication of the physical restraints; however, in more severe cases, strangulation has been reported. Moreover, the negative impacts of restraints is not limited to patients only, instead the healthcare professional have reported to experience fear, guilt and conflict when applying restraints3. Not surprisingly, the use of physical restraints is also highly prevalent in Hong Kong, with an increasing trend reported over a period of 11 years by Lam et al., (2017) who performed an observational study with data obtained from the Hong Kong Longitudinal Study on long-term care facilities (LTCF) residents between 2005 and 2015.
The study included data from 2,869 older adults and showed there was an increased use of physical restraints from 52.7% to 70.2% during this period. Notably, the use of physical restraint was independently associated with older age, impaired activities such as daily living, or cognitive function, bowel and bladder incontinence, dementia, and negative mood4. Authors recommended an appropriate healthcare staff education and policy change urgently to reduce the ever-rising reliance on such practice in the clinical setting4. But is physical restraint as bad as it sounds? The answer to this is yes because recent study by Pan et al., (2018) has highlighted a higher incidence of delirium reported in patients who were physically restrained. In addition, they also suggested that the duration and number of restraints were positively related to delirium, thus their use, particularly in the intensive care unit (ICU) should be restricted to reduce the occurrence of delirium in ICU adult patients5.
As we know physical restraints often reduces a person’s freedom to move and these restraints include bedrails, belts in chairs, or beds, and fixed tables, all of which prevents the person from getting out freely. Even though the intention for using restraints is to prevent falls or prevent patients from removing their drips or tubes, especially in older adults with mobility issues or those with cognitive impairment secondary to dementia or delirium6. However, physical restraints may inadvertently have a negative impact on the recovery and rehabilitation of older adults in hospital. In fact, guidelines recommended that their use should be reduced or stopped, and in some countries, they are illegal in most circumstances6. But what can be done in these patients then? Well, there are interventions for preventing and reducing the use of physical restraints which includes educating staff, and promote the use of other caring strategies, as using less restrictive measures6. But what else can be used apart from physical restraint to prevent falls in confused patients?
The use of pressure sensory to replace traditional physical restraints in patients at high risk of falling may be useful as it can alert the healthcare professional if the person attempts to get up from the bed6. Recently, Duxbury et al., (2019) performed a non-randomised controlled trial evaluating the strategies to minimise the use of restraints in mental health patients. The study included 14 adults from mental health wards from seven mental health hospitals in the Northwest of England and REsTRAIN YOURSELF intervention was applied and compared with 7 control wards. In total, 1,680 restraint incidences were logged over the study period. Surprisingly, the restraint rate was significantly lower on the intervention wards during the adoption phase (6.62 events/ 1000 bed-days, 95% confidence interval [CI]: 5.53-7.72) compared to the baseline phase (9.38, 95% CI: 8.19-10.55). Interestingly, on average there was a 22% reduction in restraint use and across some wards, the reduction went down to at least 60%. In addition, the association between the ward type and study phase was statistically significant. The conclusion reached at the end of the study was that it was possible to reduce the reliance on physical restraints by implementing Six Core Strategies (Figure 1)7.
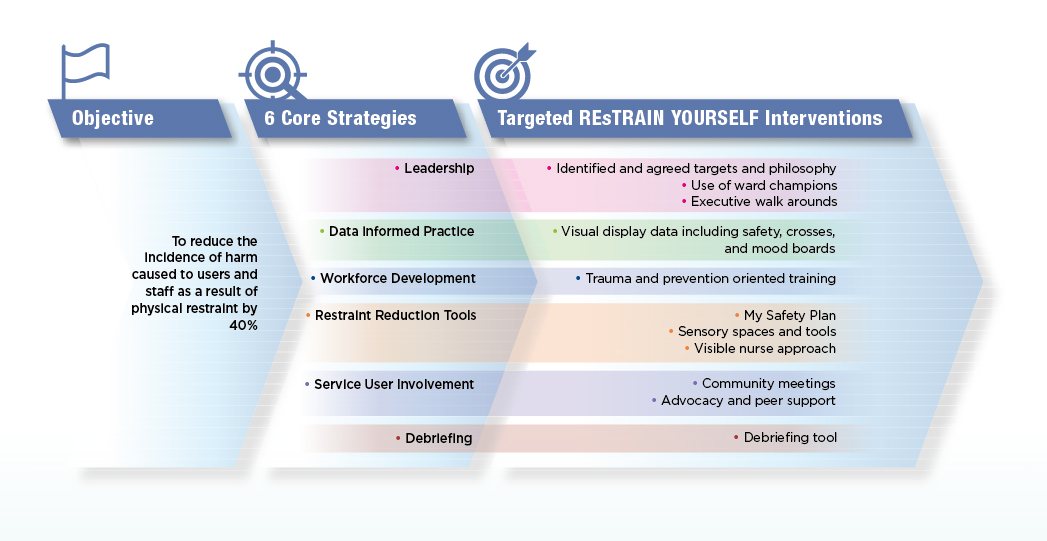
Figure 1. REsTRAIN YOURSELF interventions aligned to each of the Six Core Strategies7.
Recent studies have identified an association between physical restraint duration and undesirable outcomes among inpatients with dementia and pneumonia in acute clinical setting. One such study was by Okumura et al., (2023) who evaluated the effects of physical restraint with the discharge outcome of patients in acute clinical setting. The cohort study included a total of 18,255 inpatients with pneumonia and dementia from 307 hospitals8. Among these, 21.5% and 23.7% had physical restraint during full and partial days of hospital stays, respectively. Surprisingly, discharge to the community incidence rate was lower in the full- and the partial-restraint versus (vs) the non-restraint groups (17 vs 29 per 1,000 person-days; hazard ratio [HR], 1.79 [95% CI: 1.71-1.87]. In addition, the risk of functional decline was higher in the full-restraint vs the no-restraint groups (27.8% vs 20.8%) and the partial-resistance vs the no-restraint group (29.2% vs 20.8%). The conclusion reached towards the end of the study was that the use of physical restraints was associated with a lower incidence rate of discharge to the community and an increased risk of functional decline at discharge8. Similarly, 4-year retrospective cohort study assessing the effects of physical restraint in acute care also suggested that approximately 6% of medical patients, mostly older adults and those severely ill, were affected by restraint use9.
Are there any specific guidelines which can help healthcare professionals to determine when physical restraint can be used? The answer to this is yes there are and one such guideline was developed according to the framework of the Belgian Centre for Evidence-Based Medicine and AGREE II. The aim of this guideline was to provide an answer to six clinical questions and contained ten key recommendations based on the classification of GRADE, with the objective of increasing healthcare providers’ awareness, knowledge, and competence to adequately deal with situations or questions related to restraint use (Figure 2)10. However, in clinical practice, most of these guidelines are often under utilised and physical restraint continues to play a key role in patient management. Thus, it is important for healthcare professional to assess each patients and the situation accordingly prior, in addition to keep physical restraints as a last resort due to their detrimental effect on a patient's psychosocial health.
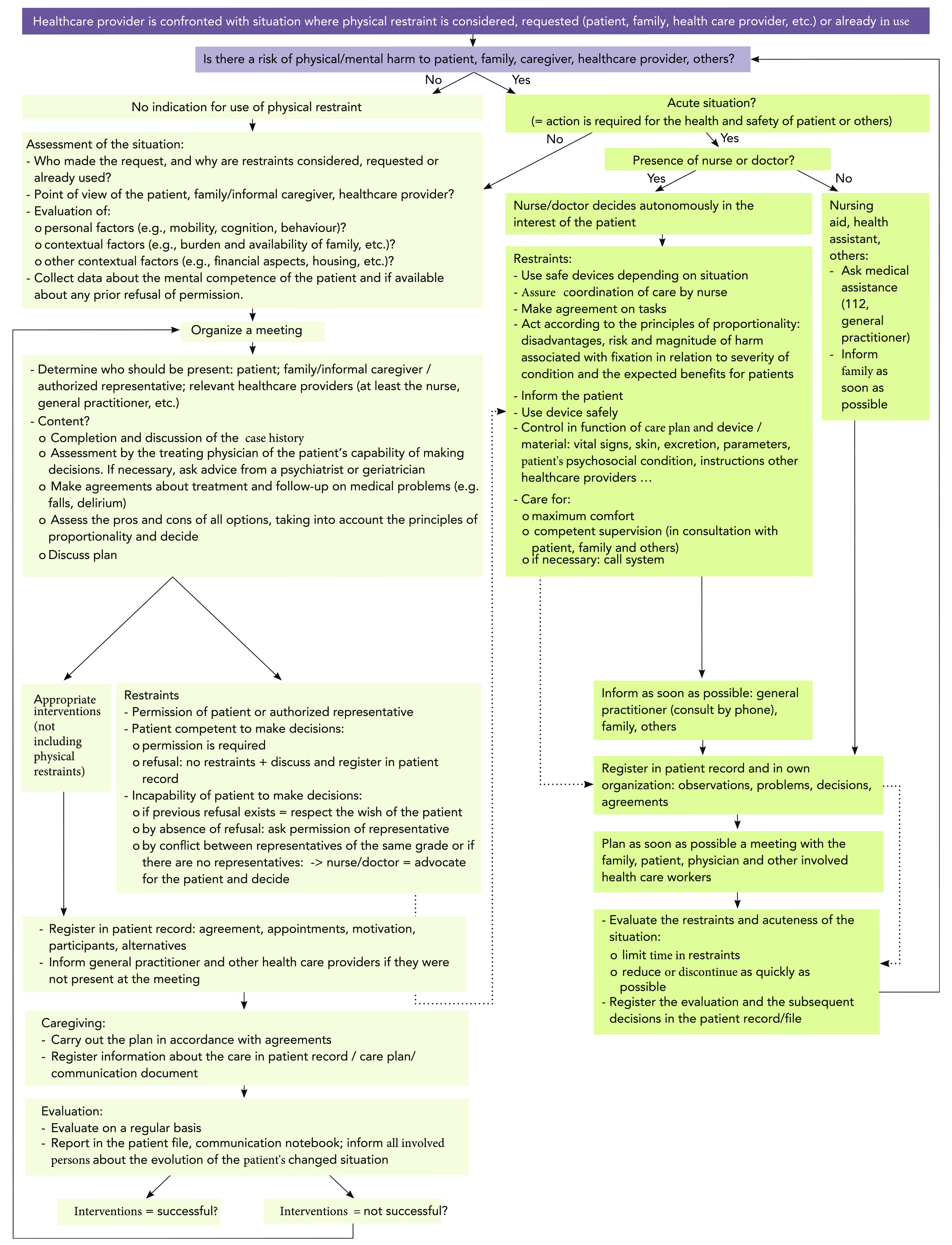
Figure 2. Flow chart of the guideline10.
References
1. Thomann S, et al. International Journal of Nursing Studies 2021; 114:103807. 2. Tang B, et al. Inquiry 2022; 59: 469580221121511. 3. Tresfon J, et al. Glob Qual Nurs Res 2023; 10: 23333936221148816. 4. Lam K, et al. J Am Med Dir Assoc 2017; 18(12): 1043-8. 5. Pan Y, et al. J Clin Nurs 2018; 27(9-10): 1950-7. 6. Abraham J, et al. Cochrane Database Syst Rev 2022; 8(8): Cd012476. 7. Duxbury J, et al. Int J Nurs Stud 2019; 95: 40-8. 8. Okumura Y, et al. J Clin Nurs 2023; 32(17-18): 6394-402. 9. Spennato U, et al. Geriatrics (Basel) 2023; 8(1). 10. Scheepmans K, et al. BMC Geriatr 2020; 20(1): 169.