Specialist in Neurology
Emeritus Professor,
Department of Medicine and Therapeutics
The Chinese University of Hong Kong
Roles of B Vitamins in the Nervous System
B vitamins are essential for the nervous system and deficiencies in one or more of these vitamins are linked to increased risks of many neurological diseases1. However, among the eight B vitamins, human epidemiological and controlled trial investigations have focused almost exclusively on the roles that a trio of B vitamins – folate B9, cobalamin B12 and pyridoxine B6 – play in metabolism of the toxic amino acid homocysteine2. In fact, hyperhomocysteinaemia has been found to be associated with several neurological and even cardiovascular conditions3. In this interview, Prof. Ka Sing Lawrence Wong revealed the roles of these B vitamins in the nervous system and shared his insights into how to manage the deficiencies.
The B Vitamins
The B vitamins are a collection of eight water-soluble, chemically very heterogeneous organic compounds. They function as coenzymes for enzymatic reactions in different biological systems. Their collective effects include energy production, synthesis and repair of DNA/RNA, genomic and non-genomic methylation, and synthesis of numerous neurochemicals and signalling molecules1, 2. However, as Prof. Wong stated, human epidemiological and controlled trial investigations have focused almost exclusively on a trio of B vitamins – folate B9, cobalamin B12 and pyridoxine B6, all of which are involved in the metabolism of the potentially toxic amino acid homocysteine2.
Biochemistry and Function of Folate, Cobalamin and Pyridoxine
Folate and cobalamin play complementary roles in the folate and methionine cycles, regenerating methionine from homocysteine (Figure 1)2. When methionine is in excess, it can be converted into cysteine, via series of intermediate steps requiring pyridoxine as a cofactor, ultimately leading to the synthesis of the potent endogenous antioxidant glutathione1-3.
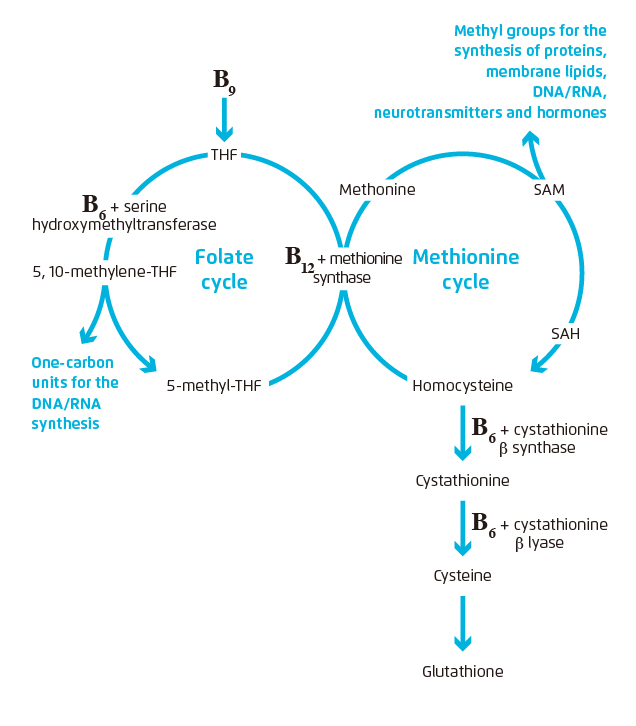
Figure 1. The folate and methionine cycles.1- 3
SAH: S-adenosylhomocysteine;
SAM: S-adenosylmethionine; THF: tetrahydrofolate
Also, cobalamin plays a role in conversion into succinyl CoA from methylmalonyl CoA (Figure 2)1. The conversion is necessary for myelin synthesis4. Pyridoxine, on the other hand, functions as a coenzyme in the synthesis of neurotransmitters needed for synaptic transmission1, 2.
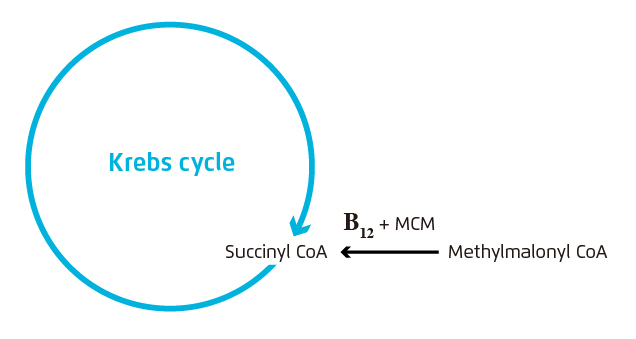
Figure 2. Conversion from methylmalonyl CoA into succinyl CoA – an important intermediate of the Krebs cycle
(a series of chemical reactions that generate energy, in the form of ATP, in the mitochondria) – with cobalamin1, 2.
MCM: methylmalonyl CoA mutase
Neurological Manifestations of Folate, Cobalamin and Pyridoxine Deficiencies
Generally, sufficient folate, cobalamin and pyridoxine can reduce levels of homocysteine, while deficiencies in these B vitamins can cause increased homocysteine levels1, 3. Hyperhomocysteinaemia is associated with an increased risk of stroke, cognitive decline and mood disorders1, 3, 5.
As pointed out by Prof. Wong, a deficiency in cobalamin alone can result in a functional folate deficiency. A functional folate deficiency not only hamper neuronal differentiation and repair, and promote hippocampal atrophy and demyelination, but also compromise the integrity of membrane phospholipids, impairing the propagation of action potentials2. Also, lack of cobalamin can lead to a decrease in normal myelin synthesis and incorporation of abnormal fatty acids into neuronal lipids. Common neurological manifestations associated with cobalamin deficiency include neuropathy, myelopathy, neuropsychiatric abnormalities, dementia, optic nerve atrophy, and subacute combined degeneration (SCD) of the spinal cord4.
Since the synthesis of neurotransmitters is differentially affected by the levels of pyridoxine, greater depletion of some neurotransmitters would occur even with mild deficiency, thereby resulting in imbalances between the levels of different neurotransmitters1, 2. Neurological manifestations of pyridoxine deficiency include impaired cognitive function, convulsive seizures, depression, carpal tunnel syndrome and peripheral neuropathy1.
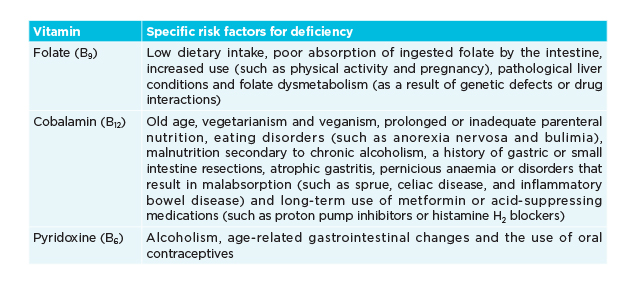
Table 1. Specific risk factors for deficiencies in B vitamins1, 6-9
Management of Deficiencies in B Vitamins
Owing to widespread food fortification with folate, cobalamin deficiency is a much more common cause of hyperhomocysteinaemia than folate deficiency in developed countries8. To avoid causing SCD of the spinal cord, cobalamin deficiency must be treated first if cobalamin deficiency coexists with folate deficiency10.
Most patients with clinical cobalamin deficiency have malabsorption and will require parenteral or high-dose 1,000 to 2,000 µg oral replacement. Adequate supplementation can achieve resolution or improvement in myelopathy and megaloblastic anaemia11. However, as told by Prof. Wong, cobalamin must be converted into active forms before it is used by the body. “Methylcobalamin is the active form of cobalamin that acts as a coenzyme for methionine synthase involved in the conversion of methionine from homocysteine and may therefore be a better treatment for cobalamin deficiency than inactive forms such as cyanocobalamin,” added Prof. Wong. In fact, a meta-analysis of individual patient data from trials of cobalamin therapy has indicated that patients with impaired renal function exposed to high-dose cyanocobalamin do not benefit from therapy with B vitamins for preventing stroke5.
In general, patients with a reversible cause should be treated until the deficiency is corrected and symptoms resolve, while treatment for those with an irreversible cause should be continued for life8, 10. As advised by Prof. Wong, for patients on long-term metformin or acid-suppressing medications, increased screening and vigilance of cobalamin deficiency and the use of oral cobalamin could be considered. In fact, cobalamin supplementation has been advocated as a prophylactic measure in vegetarians, gastrectomised patients, patients undergoing high-flux haemodialysis, and infants born to mothers with pernicious anaemia4.
Pyridoxine deficiency always coexists with deficiencies of other B vitamins such as folate and cobalamin. The vitamin is available therapeutically in both oral and parenteral formulations in illnesses linked to pyridoxine deficiency. However, the formulation and dosage used both depend on the severity of symptoms12.
References
1. Calderón-Ospina CA and Nava-Mesa MO. CNS Neurosci Ther. 2020;26:(1)5-13. 2. Kennedy DO. Nutrients 2016;8:(2)68. 3. Mitchell ES, et al. Neurosci Biobehav Rev 2014;47:307-320. 4. Briani C, et al. Nutrients 2013;5(11):4521-4539. 5. Spence JD, et al. Lancet Neurol 2017;16(9): 750-760.6. Scaglione F and Panzavolta G. Xenobiotica 2014; 44(5):480-488. 7. Kumar N. Handb Clin Neurol 2014;120:915-926. 8. Langan RC and Goodbred AJ. Am Fam Physician. 2017;96(6):384-389. 9. Morris MS, et al. Am J Clin Nutr 2008;87(5):1446–1454. 10. Hunt A, et al. BMJ. 2014;349:g5226. 11. Stabler SP. N Engl J Med 2013;368(21):149-160. 12. Brown MJ and Beier K. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019-.