Associate Consultant (Nephrology)
United Christian Hospital
Honorary Clinical Assistant Professor
The Chinese University of Hong Kong
Chronic kidney disease (CKD) is a major public health problem with substantial disease burdens. Without proper control, CKD may eventually lead to end-stage renal disease (ESRD) and various complications, including cardiovascular diseases1. Avoiding high protein intake is a main part of the nutritional treatment for non-dialysis CKD2. While some advocate low protein diet (LPD), a major possible drawback related to LPD is the increased risk of protein-energy wasting (PEW). In this regard, supplementation with ketoanalogues would allow to maintain of a good nutritional status for CKD patients on LPD.
As kidney function declines, the health of CKD patients can be impaired by the accumulation of metabolic waste products and excessive electrolytes. In this regard, nutritional management of CKD, which involves balancing the intake of energy, protein, minerals, and fluid, is essential to control uremic symptoms and slow down the progression of kidney dysfunction3. Particularly, it has been widely reported that restricted protein diet can ameliorate albuminuria, reduce the rate of kidney dysfunction, and postpone renal replacement therapy (RRT)4.
According to the Kidney Disease: Improving Global Outcomes (KDIGO) guidelines, maintaining a protein intake of 0.8 g/kg body weight/day in adults with CKD stage 3–5 is recommended. In contrast, a high protein intake (>1.3 g/kg body weight/day) should be avoided in these patients2. Practically, the daily protein intake under conventional LPD is 0.6-0.8 g/kg body weight4. Dr. Chan Zi, Associate Consultant (Nephrology) of the United Christian Hospital, added that a very low–protein diet (VLPD, 0.3-0.4 g/kg body weight/day) supplemented with ketoanalogues under close supervision can be prescribed in CKD patients who are at risk of kidney failure2.
Although LPD plays a central role in the nutritional management for CKD patients, the highly restricted renal diet may expose the patients to a higher risk of insufficient nutrient intake and PEW, which is the loss of body store of proteins and energy reserves5. More importantly, it has been reported that many non-dialysis CKD patients fail to adhere to the prescribed LPD6.
In discussing the major factors hindering adherence to LPD in local settings, Dr. Chan highlighted the influence of dietary pattern and dine out habit among local population. “Hong Kong's cuisine is heavily influenced by the Cantonese and other Chinese culinary traditions, which often feature dishes with significant amounts of protein-rich ingredients,” she noted. For instance, while roast suckling pig, barbequed pork, and brine-soaked duck are representative dishes in Cantonese cuisine, their protein contents are high7.
Apart from the protein contents in food, dine out habit among local people also hinders proper protein intake. “Under the fast-paced lifestyle and tight working schedule, dining out is more convenient,” Dr. Chan opined. Essentially, the processed food in restaurants often do not meet the balanced diet standard due to excess energy, protein, fat, and salt7.
Dr. Chan emphasised that LPD should only be recommended to metabolically stable patients who do not have any active inflammatory, infectious diseases, poorly controlled diabetes, malnutrition, or consumptive diseases, such as cancer. Therefore, patient selection is important in planning LPD for patients to enhance their adherence and reduce the risk of insufficient nutrient intake.
Existing literature advocated that managing CKD by a multidisciplinary team of healthcare professionals improves patient outcomes8. In the context of nutritional management, Dr. Chan recommended that the selected patients for LPD should be referred to renal dietitians who tailors the optimal dietary plan for the patients based on their specific conditions, such as CKD stage, comorbidity, and activity level. Moreover, dietitians would educate the patients about the essence of LPD and practical issues in controlling protein intake. In particular, Dr. Chan reminded that CKD patients on LPD should be regularly followed up by nephrologists to assess the nutritional status.
While LPD might lead to essential amino acid (EAA) deficiency, low energy intake, and an increased risk of PEW, ketoanalogues of EAA can serve as substrates for protein synthesis without the production of toxic nitrogenous waste products. Hence, supplementation with ketoanalogues allows a reduced intake of protein while lowering the risk of adverse impacts of inadequate dietary protein intake9.
Dr. Chan stated that, currently, there are evidence suggested that supplement with ketoanalogues to LPD or VLPD can slow down CKD progression4,10. For instance, the meta-analysis by Chewcharat et al. (2019), which included 17 randomised controlled trials (RCTs) accounting for 1,459 CKD patients, indicated that restricted protein diet with ketoanalogues significantly preserved renal function, improved blood pressure, and CKD-Bone Mineral Density parameters. Notably, the results further showed that VLPD with ketoanalogues was superior to LPD with ketoanalogues in slowing the decline in eGFR4.
More recently, a retrospective cohort study involving 1,042 CKD patients by Ariyanopparut et al. (2023), suggested that, during a median follow-up of 32.9 months, patients with LPD with ketoanalogue had a significantly lower primary outcome, which was either a rapid eGFR decline or commencing dialysis, (6.1 per 1000 person-months) compared to those with LPD alone (18.3 per 1000 person-months, p<0.001, Figure 1). Also, LPD with ketoanalogue yielded a significantly lower risk of kidney function decline (hazard ratio [HR]: 0.13, p<0.001) and dialysis initiation (HR: 0.24, p<0.001) than LPD alone after adjusting for confounders. Remarkably, the annual rate of eGFR decline in patients receiving LPD with ketoanalogue was 4.5 ml/min/1.73m2, which was significantly lower than that with LPD alone (7.7 ml/min/1.73m2, p=0.001)11.
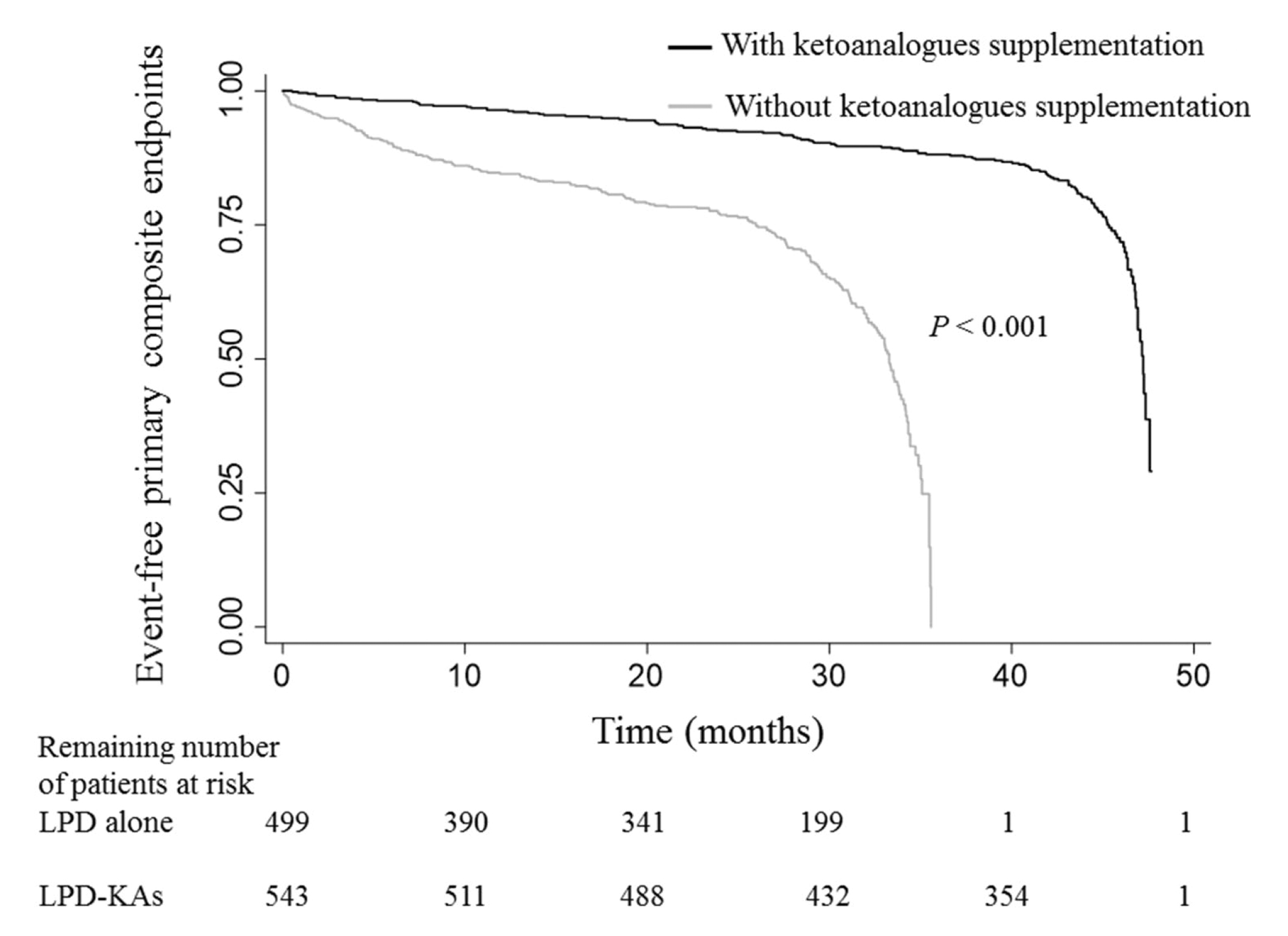
Figure 1. Kaplan–Meier estimates of primary composite endpoint in CKD patients on LPD with/without ketoanalogues supplementation11
The study postulated in addition to nutrition supplement, ketoanalogues can prevent dysfunctional amino acid synthesis during protein restriction and it may also have direct renoprotective effect by enhanced endothelial function.
Recently, an abstract by Dr. Chan and co-workers (2024), involving local patients with stage 4-5 CKD on LPD, reported that the addition of ketoanalogue resulted in a trend of slowing CKD progression.
The study was a retrospective cohort study included 15 local CKD stage 4-5 patients on LPD. The patients were provided with ketoanalogue treatment for a total duration of ≥6 months. The slopes of eGFR before and after ketoanalogue supplementation were calculated while responders were defined as patients who showed decreased eGFR slope upon ketoanalogue supplementation12.
By comparing the pre- and post-treatment slopes of eGFR, additional ketoanalogue treatment to LPD showed a trend of slowing CKD progression (-0.398±0.466 vs -0.122±0.374, p=0.117). The trend did not reach statistic significant may probably be due to the small sample size and relatively short follow-up time.
There were 10 responders to ketoanalogue treatment identified, whereas older age was indicated to be a significant predicting factor of treatment responses (independent sample t-test, p=0.046)12. In discussing the possible reasons for older age in predicting response to ketoanalogue treatment,
Dr. Chan postulated that older people may have a lower protein intake or more likely to comply with the prescribed LPD than the younger counterparts, due to lifestyle and cultural factors. Besides, she opined that the differences in CKD aetiology between older and younger people may also contribute to the varied outcomes. Further larger-scale investigations with longer treatment duration are needed to confirm the clinical benefits.
Apart from restricted protein diet with ketoanaloges, Dr. Chan advised that CKD patients are encouraged to adopt healthy and diverse diets, whereas plant-based foods are more preferable than animal-based ones. “A plant-based diet is rich in anti-inflammatory nutrients, fibres, and phytochemicals, and it has been shown to reduce proteinuria and decrease metabolic acidosis,” she commented. Essentially, CKD patients should maintain an adequate caloric intake to prevent malnutrition. For patients with stable CKD, 25-35 kcal/kg body weight per day is need in general, based on age, sex, level of physical activity, body composition, weight status goals and CKD stage13. Particularly, Dr. Chan reminded that CKD patients should avoid ultra-processed foods, such as sweetened beverages, fast foods, frozen meals, chips, candy, and pastries, since these foods can promote inflammation and may worsen kidney function.
In conclusion, restricted protein diet supplemented with ketoanalogues has been demonstrated to effectively delay CKD progression. Given that most existing studies on restricted protein diet with ketoanaloges included primarily CKD stage 3-5 patients, further investigations on its benefits for earlier stage CKD are highly desirable.
References
1. PCouser et al. Kidney Int 2011; 80: 1258–70. 2. Stevens et al. Kidney Int 2024; 105: S117–314. 3. Kim and Jung. Korean J Intern Med 2020; 35: 1279. 4. Chewcharat et al. J Ren Nutr 2020; 30: 189–99. 5. Bellizzi et al. BMC Nephrol 2018; 19: 1–11. 6. Cupisti et al. Journal of Clinical Medicine 2020, Vol 9, Page 3644 2020; 9: 3644. 7. Zhang et al. Journal of Ethnic Foods 2020; 7: 1–10. 8. Collister et al. Can J Kidney Health Dis 2019; 6. DOI:10.1177/2054358119882667. 9. Bellizzi et al. Nutrients 2022; 14. DOI:10.3390/NU14030441/S1. 10. Garneata et al. J Am Soc Nephrol 2016; 27: 2164–76. 11. Ariyanopparut et al. Sci Rep 2023; 13: 15459. 12. Chan et al. APCN & KSN 2024; : A0373. 13. Ikizler et al. Am J Kidney Dis 2020; 76: S1–107.